Case: Repeated Episodes of Periodic Paralysis
Neha Pradeep, MBBS 9th semester
Roll no: 99
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
Following is the view of my case :
(history as per the date of admission)
Case:
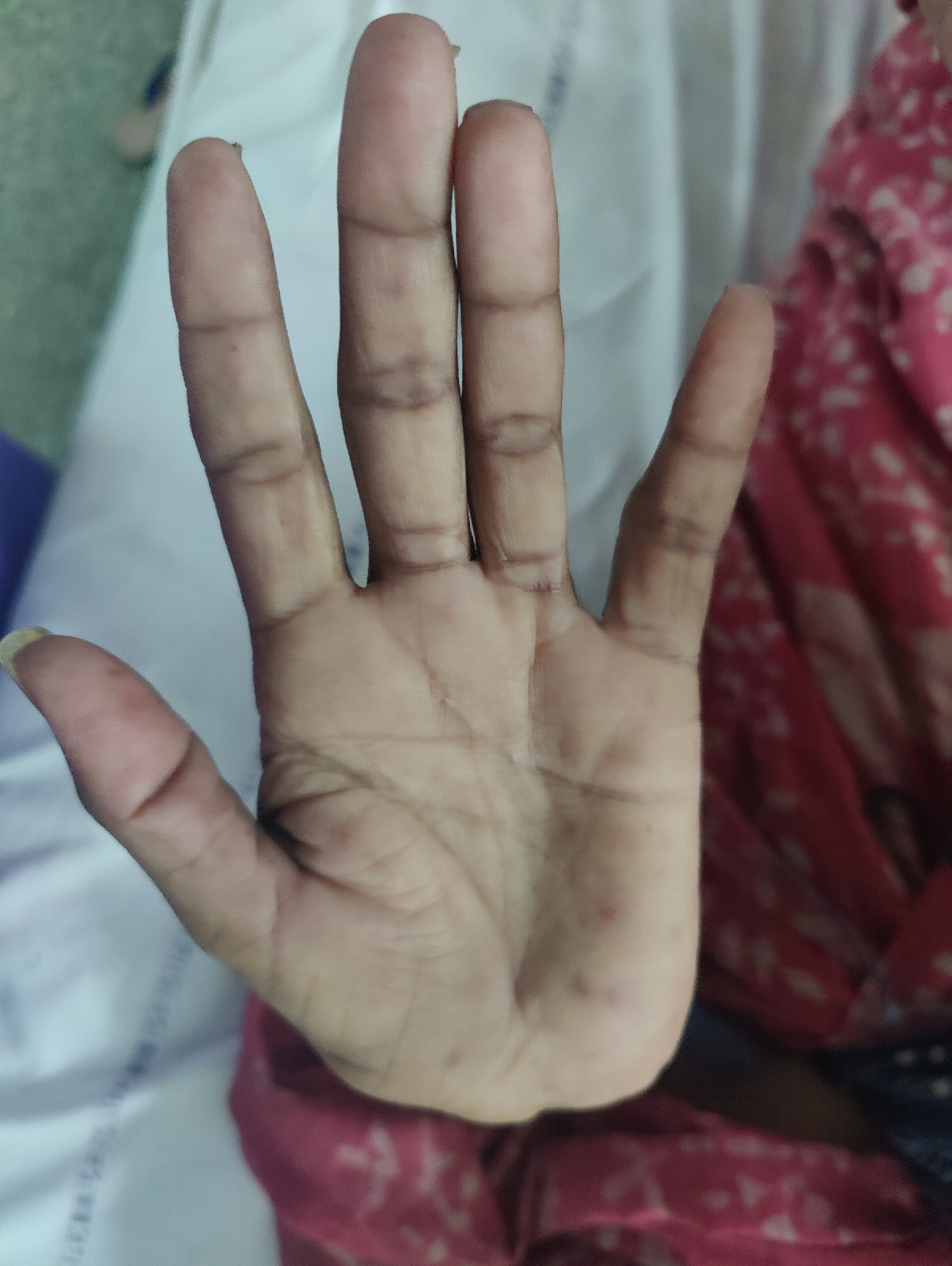
A 62 year old male presented with weakness in both lower limbs extending upto thigh unable to lift and walk.
History of Presenting Illness:
Patient came with the complaint of weakness in both lower limbs and upper limbs one day ago.
He came with a mild fever since one day.
The weakness was not progressive.
He had consumed alcohol before going to sleep, from which he woke up and felt the weakness.
Past history:
He is the eldest of 5 sons and owns 4 acres of land, grows rice and owns and drives a tractor to plough the field.
5 years ago, on an occasion, he was made to drink herbal medication in order to make him quit drinking. He developed fever the same night with chills and was taken to hospital and he even recollects that his voice was getting low and starting from paralysis of lower limbs in an ascending manner and was referred to Kims, Narketpally. He stayed for 3 days and was discharged on potassium supplementation.
6-10 days later he developed paralysis of lower limbs and was again brought to Kims, Narketpally, and was corrected and was symptom free for one month.
He developed paralysis for third time later, after 1-2 months. He was taken to Gandhi hospital for the same complaint and was treated there. He recovered and was symptom free for 4 years.
He discontinued the medication from 2 yrs and presented to our hospital
Personal history:
Diet: Mixed
Appetite: Normal
Bowel and Bladder: Regular
Sleep: Adequate
Allergies: None
He is an alcoholic since 30 years , daily intake (90-180 ml whisky) and denies smoking.
No history of Diabetes Mellitus, Hypertension, and Coronary Heart Disease.
General Exam:
Patient is concious, coherent and cooperative.
Moderately built and well nourished
No pallor , cyanosis, clubbing , lymphadenopathy, edema.
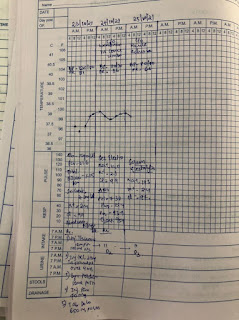
Vitals-
PR- 90 bpm
BP- 110/80 mm hg
Rr- 20 cpm
Spo2 - 98% at ra
Systemic examination:
Cvs- s1,s2 +
RS- BAE+
P/a - soft ,non tender, bs+
Cns-
RL LL
Tone: UL- N N
LL- N N
Power UL- +4 +4
LL- + 3 +3
Reflexes
B +1 +1
T +1 +1
S +1 +1
K + 1 +1
Plantar - Flexor Flexor









Comments
Post a Comment