Pre-final Case: 31 year old female with fever and joint pains
Neha Pradeep
9th Semester
Roll no. 99
Patient was apparently asymptomatic 2 years ago (March 2020)
She then developed pain in her right shoulder because of which she could not raise her hand above her shoulders. It was dull aching type and continuous, for which she went to an Orthopaedic and was given medication. The pain kept alternating between right and left shoulder and sometimes both simultaneously. She then experienced tightness of shoulder joints on waking up and needed someone to pull her up from the bed. Her pain was relieved on medication though it kept recurring for 6 months.
One month later she noticed swelling in the proximal interphalangeal joints. It was associated with decreased function. She was not able to write properly, open bottle cap or close a tap.
She also developed bilateral knee pains and generalized weakness.
Then she developed fever, oral ulcers , redness of eyes, diminished vision, and facial puffiness. She then went to a private hospital.
She developed hair loss 2 years ago, which was gradually progressive.
On routine investigations, nephrotic range proteinuria was detected in her urine sample, increased protein creatinine ratio of 4.99 due to which they decided to a kidney biopsy.
BIOPSY FINDINGS: focal mild increased endocapillary cellularity pointing towards FOCAL GLOMERULONEPHRITIS
ANA PROFILE: Anti -RNP/ Sm and Anti- Sm, Anti-Jo 1, Anti - ds DNA, nucleosomes and RIBOSOMAL P- PROTEIN were present.
Based on this the diagnosis of SLE was made.
She was prescribed Tab. OMNOCORTIL 5mg for 3 days, which was tapered over 6 months to 2.5mg.
After 6 months, steroids were stopped and was started on
- Tab. MMF for 4 months (2 tab at 8 AM and 1 tab at 8 PM),
=> Which she used and stopped after one month after tapering.
=> She was also advised to perform exercises.
In January 2022,
- She was started on FOLITRAX after which she noticed increase in number of oral ulcers, so she went to a private hospital 15 days later, and was started again started on OMNOCORTIL 5mg.
At present, the patient is complaining of bilateral knee pains since two weeks, aggrevated since last 3 days, associated with difficulty in walking and getting up when sitting. Pain is worse in the morning.
Fever since two weeks, low grade initally and progressive. Not associated with chills and rigors. Relieved on medication. Not associated with vomiting, diarrhoea, cough and cold.
Oral ulcers since 6 months, aggregated since last three months because of which the patient is unable to eat comfortably. There has been weight loss of 6 kgs in the last 3 months. No bleeding or discharge from the ulcer.




Pain in the left hypogastrium and epigastrium after eating. Two episodes of vomiting last night, watery consistency, no good particles.

- Tab. MMF 500mg PO BD (8AM & 8 PM)
- Tab. FOLITRAX 10mg weekly once
- Tab. LIVOGEN PO BD
- TAB. HCQ 200mg OD
- Tab. SHELCAL PO OD
- Tab. THYRONORM 50mcg



Upto 31/03/22











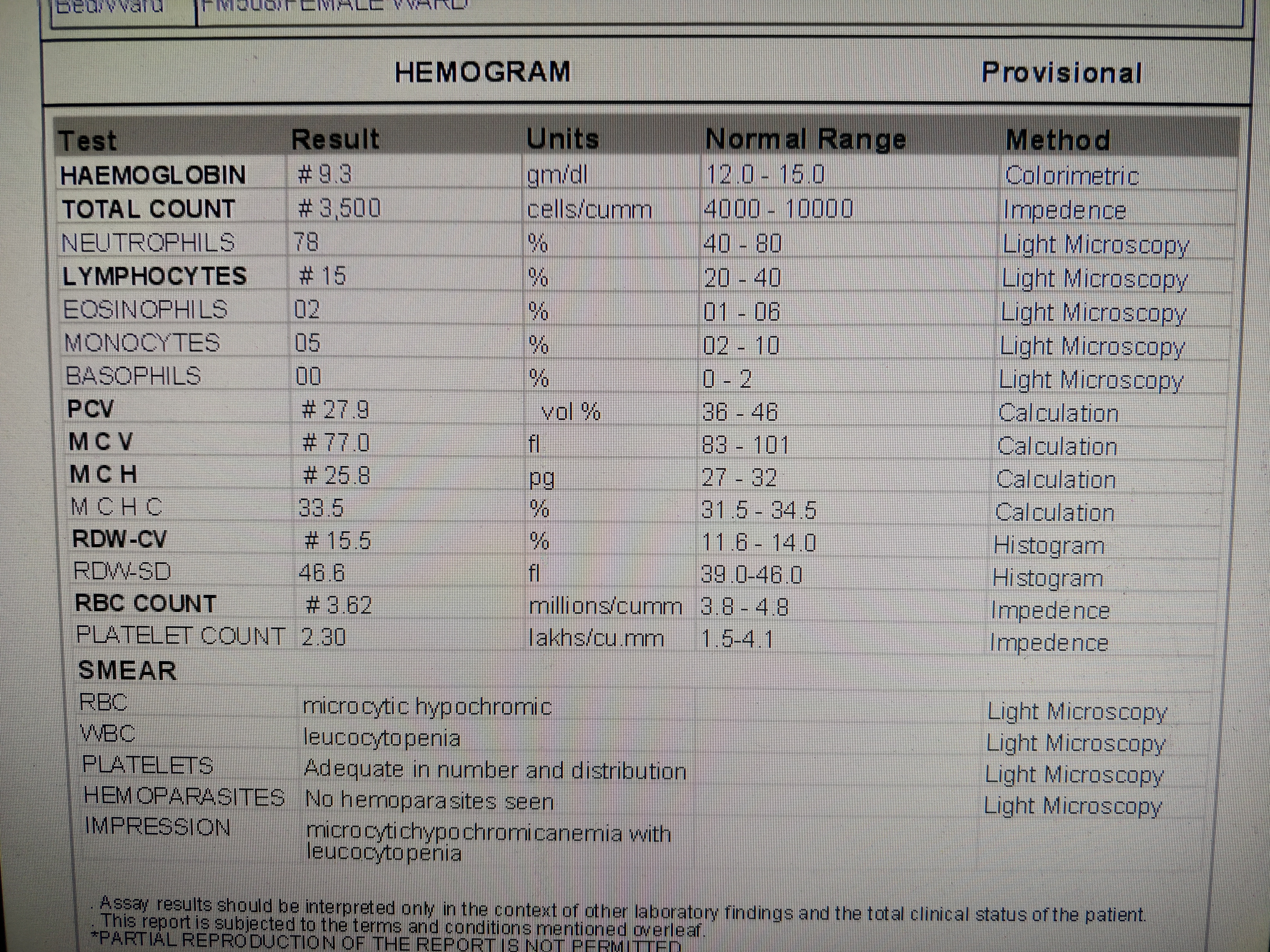
Laboratory Investigations:


- IVF NS RL @ 75ml/hr
- Inj. NEOMOL 1 gm IV SOS
- Tab. DOLO 650mg PO/QID
- MUCOPAIN GEL for L/A over ulcers.
- Tab. MMF 500mg PO BD (8AM & 8 PM)
- Tab. FOLITRAX 10mg weekly once
- Tab. LIVOGEN PO BD
- TAB. HCQ 200mg OD
- Tab. SHELCAL PO OD
- Tab. THYRONORM 50mcg









Comments
Post a Comment