57/M with ALTERED SENSORIUM 2⁰ HYPOGLYCEMIA
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
CHIEF COMPLAINTS and HOPI
A 56 year old male patient who is a resident of koilagudem (nalgonda district)who is a daily wage labourer by occupation brought to the casualty in unresponsive state at 1:30 Am .patient was found drowsy from 1 pm on 25/04/2023 And suddenly developed seizure like activity associated with slurring of speech,uprolling of eyeballs,stiffness of all four limbs,
Associated with involuntary defecation and micturition and found unresponsive.
No h/o fever ,cough.
No h/o neck stiffness and projectile vomitings.
No h/o generalised weakness ,tingling,numbness.
No h/o head trauma.
Cheif complaints of swellings with discharge not associated with pain on the left forearm. History of similar swellings with discharge on and off from past 6 months.
PAST HISTORY:
No history of similar complaints in the past.
Known case of Diabetes type 2 since 1 month.on glimiperide 1mg and metfromin 500mg.
known case of asthma since 30 years.
Not a known case of Diabetes,HTN,Epilepsy,CAD,TB.
FAMILY HISTORY:
No similar complaints in the family.
PERSONAL HISTORY:
DIET : MIXED
APPETITE: ADEQUATE
SLEEP:NORMAL
BOWEL AND BLADDER :REGULAR
ADDICTIONS: NO ADDICTIONS.
TREATMENT HISTORY:
GENERAL EXAMINATION:
Patient is unresponsive.
Pupils dilated sluggishly reactive.
Poorly built and poorly nourished.
Vitals: Pulse rate during admission 52 bpm on atropine 98bpm.
Respiratory rate:32cpm.
Spo2 :98%@RA.
Bp:120/90MMHG
Temp:afebrile.
SYSTEMIC EXAMINATION:
CVS:S1,S2 HEARD,NO MURMURS.
RS:BAE+,NVBS.
P/A: SOFT ,NON TENDER.
CNS: Patient is unresponsive at first.
HMF:INTACT
MOTOR EXAMINATION
TONE: rt lt
UL: N. N
LL:N N
REFLEXES:
B:2+ 2+
T:2+ 2+
S:2+ 2+
K:2+ 2+
A2+ 2+
P:2+ 2+
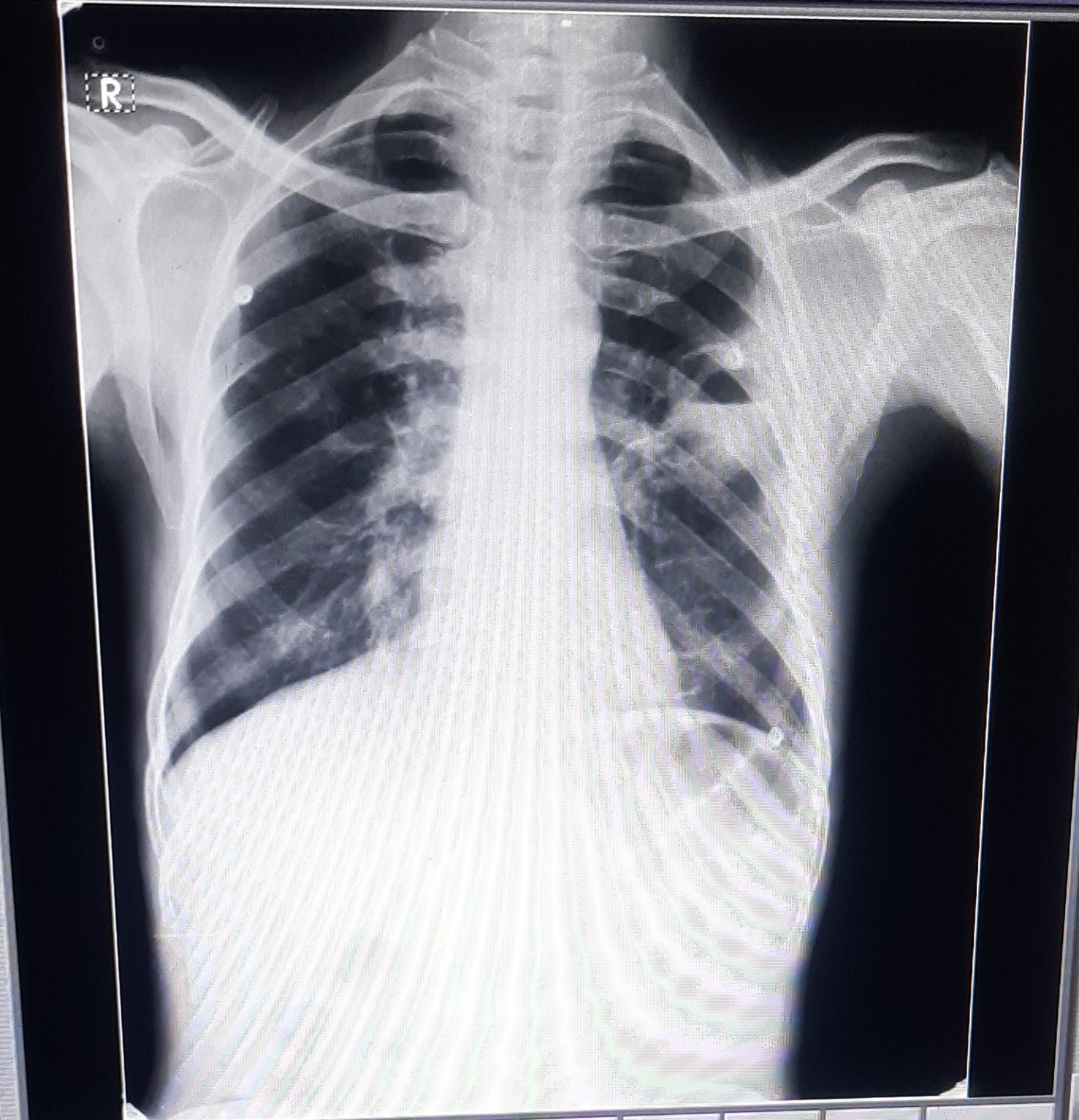
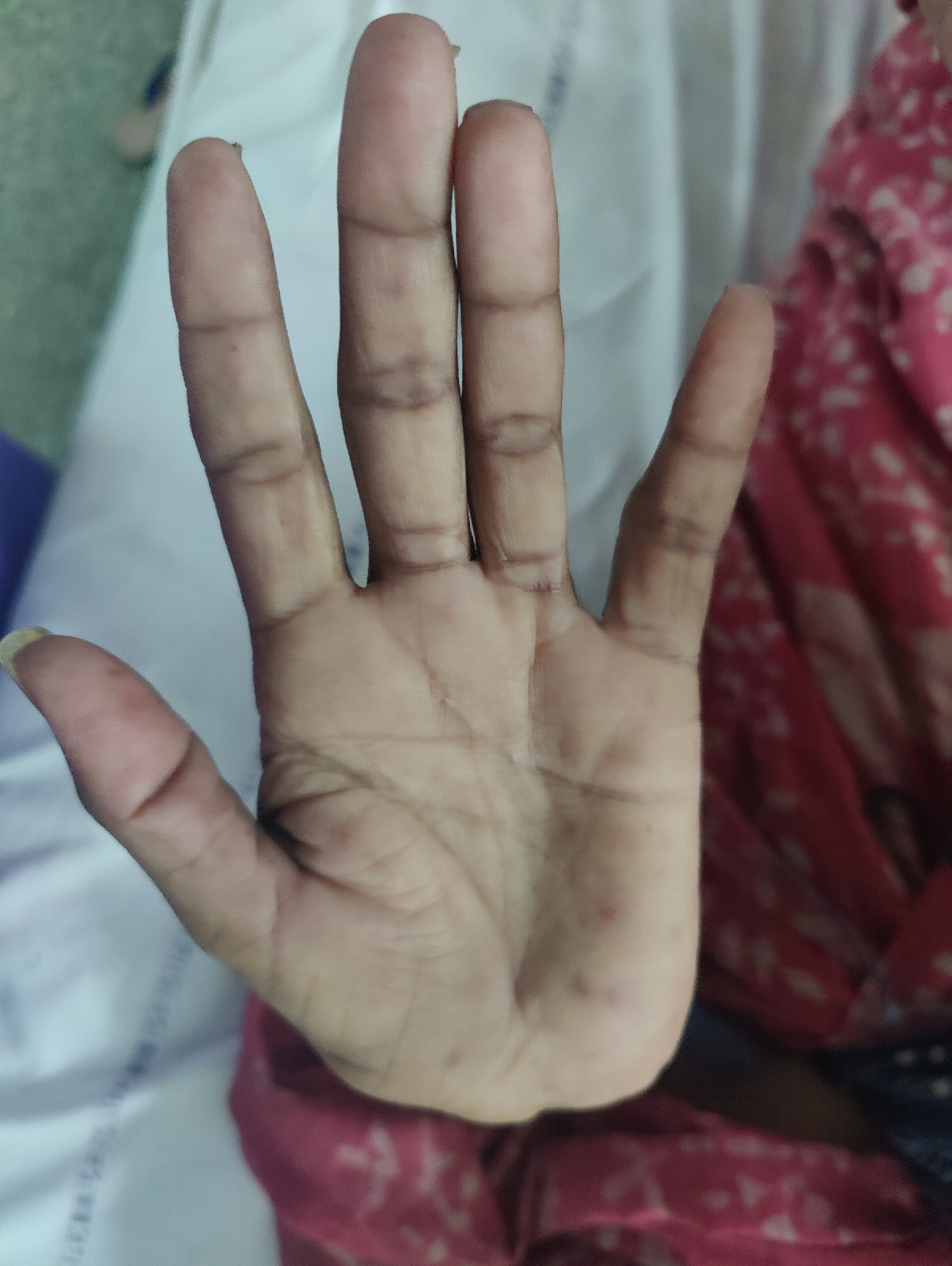
INVESTIGATIONS AND CLINICAL IMAGES:






















HACHETS FACIES:
Frontal balding .
Atrophy of temporalis muscle.




PROVISIONAL DIAGNOSIS:
ALTERED SENSORIUM SECONDARY TO ?HYPOGLYCEMIA.
Treatment:
1IVF NS @@ 50ml/hr.
2.Inj:25%DEXTROSE INFUSION @10ml/hr
Increase/decrease according to GRBS.
3.INJ:PIPTAZ 4.5 g/Iv/TID
4.Inj.CLINDAMYCIN TID
5.TAB.DOLO 650 mg/po/(sos)


Comments
Post a Comment