45/M with CKD ON MHD since 2 years
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
CHIEF COMPLAINTS:
45 year old male, resident of Rajavaram came with complaints of - decreased urine output 2 years back
-facial puffiness 2 years back
-swelling of feet 2 years
HOPI:
Patient was apparently asymptomatic two years back and then he had complaint of bilateral pedal edema which was grade 2 a/w decreased urine output where he would not pass urine even once per day. It was also associated with shortness of breath on doing daily activities.
He went to a local hospital and was diagnosed to have Renal Failure and started on Maintainence Hemodialysis. He was refered to our hospital to continue the treatment.
Since 15 days the patient has been having episodes of fever, high grade, incidious in onset, no diurnal variation, relived on medication, not associated with burning micturition, nausea, vomitings, headache or loose stools.
Past history:
K/c/o HTN since 2 years
K/c/o DM2 since 2 years
K/c/o hypothyroidism since 1year 4months
On regular medication for all 3
N/K/C/O asthma, tb, epilepsy, CAD
Personal History:
Appetite: Normal
Diet: Non-veg
Bowel: Regular
Bladder: Decreased frequency
Sleep: Adequate
Addictions: Occassionally alcoholic
Family History:
Insignificant
General examination:
Patient was conscious, he was dazed and irritable and so history was taken from attender
Pallor- Present

icterus- absent
cyanosis- absent
clubbing- absent
Lymphadenopathy - absent
Edema- B/L pedal edema present, pitting type

Vitals
Temp: 98.1
BP: 100/60
PR:94 bpm
RR: 24 cpm
sPO2: 98% at RA
Edema of the right hand noted. Pulse and BP were not palpable in this arm.
The swelling was upto elbow, present since 6 days, tender.


Systemic Examination:
CVS:
S1 and S1 sounds were heard.
No murmurs.
Respiratory System:
BAE +
Per abdomen:
Soft, non-tender
No organomegaly
CNS:
NFND


01/04/23:
Ascitic tap done, cytology report impression:
No evidence of atypical cells.
Negative for malignancy.
09/04/24:


10/04/23:

After Dialysis Arrest:

25/04/23:








USG on 25/04/23:
Impressions:
1. Gross ascites with loculation
2. Thickened sludge in gall bladder
3. Minimal right pleural effusion
4. Grade II RPD changes in bilateral kidneys
10/05/23:


11/05/23



11/05/23
SOAP notes:
S
Patient was put on his regular Maintainence Hemodialysis at 5 pm on 10/5/23. At 5:30 pm his BP was 120/80 mmHg. At 6 pm, the patient became unresponsive. Pulse was feeble and BP was unrecordable. GRBS was found to be 78 mg/dl. Cardiac massage was started and patient was simultaneously given a 25 D bolus, started on a Norad infusion and given oxygen.
Patient showed response and when the systolic BP came to 130, he was shifted to ICU.
O
Patient is c/c/c
Temp:- 98.4°F
PR- 119 bpm
RR-20cpm
BP- 110/70 mmHg with Norad @10 ml/hr
GRBS: 198 mg/dl
Spo2-100% at room Air
CVS- S1s2present, no murmurs heard
RS-B/L air entry present, NVBS
PA- soft,NT
CNS - NFND
GCS: E2V2M6
A
CKD on MHD ?Septic Shock ?Cardiogenic Shock ?NSTEMI (Anterolateral). Pyrexia under evaluation (resolved)
HTN +, DM +, Hypothyroidism +
Hemogram on 11/5:
Hb- 11.1 gm/dl
TLC: 25000 cells/cu.mm
PCV: 37.9 %
RBC count: 3.63 million/cu.mm
Platelets: 2.1 lakh/cu.mm
Impression: Normocytic normochromic with neutrophilic leucocytosis
Blood lactate on 11/5: 16 mg/dl
RFT on 11/5:
Urea: 129 mg/dl
Creatinine: 8.6 mg/dl
Uric acid: 10.3 mg/dl
Phosphorus: 6.6 mg/dl
P:
1)INJ. NORADRENALIN 20 ML IN 46 ML OF NS @10 ML/HR (increased or decreased to maintain mean arterial pressure more than 65 mmHg)
2)INJ. PIPTAZ 2.25 gm IV/TID
3)INJ. EPO 4000 IU S/C ONCE WEEKLY
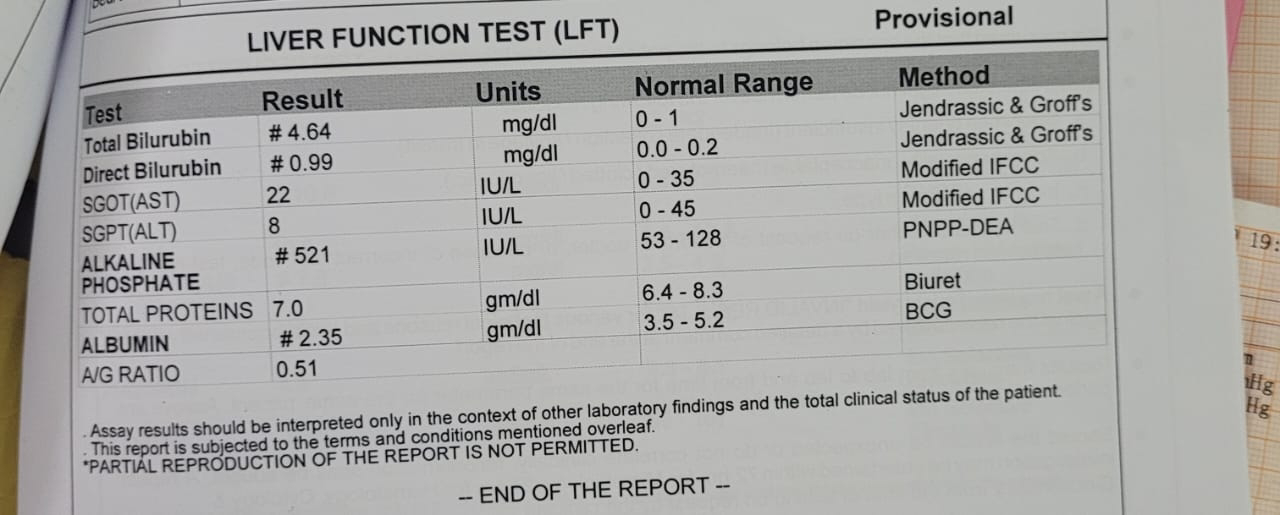
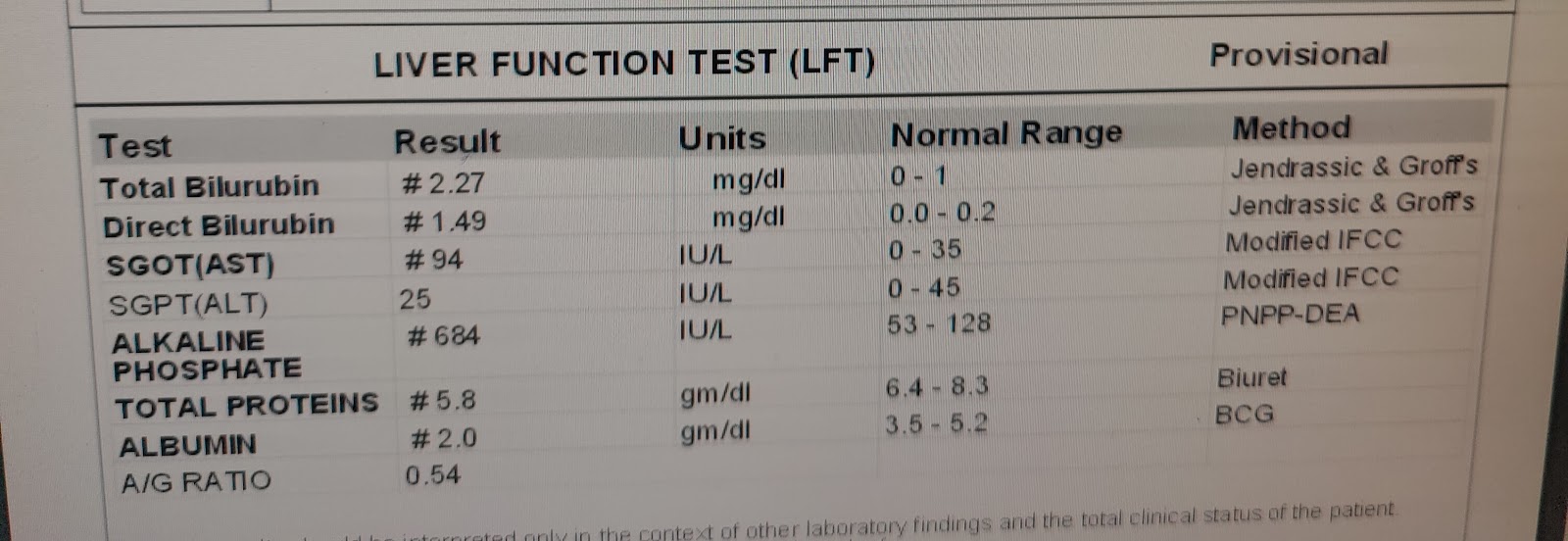
4)TAB. UDILIV 300 mg PO/BD
5)TAB. THYRONORM 50 mcg PO/OD bbf
6)TAB. ECOSPIRIN-AV (75/10) PO/HS
7)TAB. OROFER XT PO/OD
8)TAB. DOLO 650 mg PO/SOS
9)TAB. SHELCAL 500 mg PO/OD
10)SYP. CITRALKA 15 ml in 1 glass of water PO/HS



Comments
Post a Comment